
From the 1Department of Rehabilitation Medicine, Erasmus MC, University Medical Centre Rotterdam, 2Department of Rehabilitation Medicine, VU, University Medical Centre Amsterdam, 3Rijndam Rehabilitation Centre, Rotterdam, 4Department of Neurology, and 5Department of Public Health, Erasmus MC, University Medical Centre Rotterdam, The Netherlands
Objective: Despite the widespread use of botulinum toxin in ambulatory children with spastic cerebral palsy, its value prior to intensive physiotherapy with adjunctive casting/orthoses remains unclear.
Design: A pragmatically designed, multi-centre trial, comparing the effectiveness of botulinum toxin + intensive physiotherapy with intensive physiotherapy alone, including economic evaluation.
Subjects/patients: Children with spastic cerebral palsy, age range 4–12 years, cerebral palsy-severity Gross Motor Function Classification System levels I–III, received either botulinum toxin type A + intensive physiotherapy or intensive physiotherapy alone and, if necessary, ankle-foot orthoses and/or casting.
Methods: Primary outcomes were gross motor func-tion, physical activity levels, and health-related quality-of-life, assessed at baseline, 12 (primary end-point) and 24 weeks (follow-up). Economic outcomes included healthcare and patient costs. Intention-to-treat analyses were performed with linear mixed models.
Results: There were 65 participants (37 males), with a mean age of 7.3 years (standard deviation 2.3 years), equally distributed across Gross Motor Function Classification System levels. Forty-one children received botulinum toxin type A plus intensive physio-therapy and 24 received intensive physiotherapy treatment only. At primary end-point, one statistically significant difference was found in favour of intensive physiotherapy alone: objectively measured percentage of sedentary behaviour (–3.42, 95% confidence interval 0.20–6.64, p = 0.038). Treatment costs were significantly higher for botulinum toxin type A plus intensive physiotherapy (8,963 vs 6,182 euro, p = 0.001). No statistically significant differences were found between groups at follow-up.
Conclusion: The addition of botulinum toxin type A to intensive physiotherapy did not improve the effectiveness of rehabilitation for ambulatory children with spastic cerebral palsy and was also not cost-effective. Thus botulinum toxin is not recommended for use in improving gross motor function, activity levels or health-related quality-of-life in this cerebral palsy age- and severity-subgroup.
Key words: spastic cerebral palsy; botulinum toxin; physio-therapy; cost-effectiveness.
Accepted Jul 10, 2017; Epub ahead of print Sep 26, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Fabienne Schasfoort, Department of Rehabilitation Medicine, Erasmus MC, University Medical Centre Rotterdam, PO Box 2040, NL-3000 CA Rotterdam, The Netherlands. E-mail: f.schasfoort@erasmusmc.nl.
Multi-level treatment with botulinum toxin type A (BoNT-A) is widely used in spastic cerebral palsy (CP). By reducing muscle spasticity/abnormal muscle tone, BoNT-A aims to improve an individual’s activity and participation, domains related to higher level of functioning, as described in the World Health Organization’s International Classification of Functioning (ICF) (1). BoNT-A is prescribed for the majority of ambulatory children with spastic CP in most Western countries (2) and treatment is repeated frequently throughout childhood (3). BoNT-A injections are not a stand-alone intervention and should be combined with additional, preferably activity-focused, interventions (4, 5). Leg muscle injections are usually combined with physiotherapy (PT) and, if necessary, additional casting and/or ankle-foot orthoses. The rationale for this is that BoNT-A may provide better conditions to optimize and reinforce the effects of PT and adjunctive interventions in combined treatment.
In general, positive effects of combined treatment have been reported on outcomes at the ICF level of body function and structure (i.e. reducing muscle spasticity and hypertonia and improving range of motion). However, treatment effects on higher ICF levels of functioning remain unclear (4–6). Furthermore, there is a lack of clarity regarding the degree that positive outcomes of combined treatment can be attributed to BoNT-A (7–9), as a period of intensive, goal-directed PT without BoNT-A also seems to be effective (6, 10). BoNT-A treatment is burdensome (i.e. a toxin is injected, usually under anaesthesia) and costly. In addition, a potential industry-related conflict of interest regarding the effectiveness of BoNT-A has been reported recently (11). Hence, it is important to explicitly study the added value of BoNT-A in combined intensive treatment. The aim of this study was therefore to determine the effectiveness and costs of multi-level BoNT-A injections in combination with a 12-week period of intensive functional PT (BoNT-A+iPT) compared with the effectiveness and costs of a 12-week period of intensive functional PT alone (only-iPT). Primary outcomes for effectiveness were gross motor function, physical activity levels and health-related quality of life.
A pragmatically designed, single-blind, multi-centre trial was performed to compare the effectiveness of BoNT-A+iPT with only-iPT. Randomized participants and those who had objections to randomization because, for various reasons, they strongly preferred one of the interventions were both enrolled in the study. Thus, due to allowing inclusion of participants according to family preferences, this was not a fully randomized trial (12, 13) and the study was conducted pragmatically. Power calculations (performed for the originally intended fully randomized trial) were based on simulation of 500 data-sets with mixed effect model analyses (α = 0.05, β = 0.20) using existing Gross Motor Function Measure (GMFM) data (14). A total sample size of 60 children was considered sufficient. Economic evaluation was performed from a societal perspective.
Children were recruited from 2 Dutch university hospitals and 5 rehabilitation centres. During regular consultations with the spasticity-management team, experienced multidisciplinary teams of clinical professionals assessed children for eligibility. Inclusion criteria were: diagnosis of spastic CP (15), primarily lower extremity involvement (unilateral or bilateral), classified at levels I–III of the Gross Motor Function Classification System (GMFCS) (16), age range 4–12 years, and an indication for BoNT-A (4, 5). Exclusion criteria were: BoNT-A treatment < 6 months or CP-related surgery < 12 months prior to enrolment, cognitively unable to understand instructions, presence of severe contractures or co-morbidity. The ethics committee of Erasmus MC approved the study, and the trial was registered in the Dutch Trial Register (NTR TC 1655). Written informed consent was obtained from parents/primary caregivers.
Parents of eligible children were initially invited to participate on a randomized basis. If they declined, they were then offered participation in the group they preferred. The subjects who were randomized were centrally assigned to either BoNT-A+iPT or only-iPT by a computer-generated, independently provided, block randomization scheme with stratification by GMFCS level per measuring location (i.e. the university hospitals). The aim was to blind the outcome assessors, physiotherapists and those administering additional post-BoNT-A co-interventions. For randomized participants, allocation to intervention groups was concealed until after baseline measurements. Physio-therapists and outcome assessors were asked to speculate the child’s suspected intervention group after primary end-point measurements. Blinding of physiotherapists and assessors in the group that received preferred treatment was also pursued and its success similarly assessed. All data were anonymized and coded prior to data analysis, which was performed by individuals not involved with the interventions or outcome assessments.
After baseline measurements, individual BoNT-A treatment plans were compiled based on clinical examination and instrumented gait analysis. Indications for co-interventions during the iPT period (i.e. serial casting and prescription or (re)alignment of ankle-foot orthoses (AFOs)) were also determined. In the BoNT-A+iPT intervention group, BoNT-A was administered under general anaesthesia by experienced clinicians during individually scheduled 1-day hospitalizations. Treatment adhered to recommendations pertaining to preparations, cautions, dose modifiers, localization techniques and safety aspects (European Consensus 2009) (4). In all cases, preparations of botulinum toxin serotype A (Botox®, Allergan Inc., Eindhoven, The Netherlands) were used, and in each treated muscle group, the maximum allowed dose, in relation to children’s age and weight, was injected.
The period of intensive functional PT (iPT) started one week after BoNT-A for the BoNT-A+iPT intervention group, and was individually scheduled for children in the only-iPT intervention group. A guideline was developed based on best-available evidence (2010) (17, 18). During a 12-week period, children ideally had 3 45–60-min therapy sessions each week, with at least 1 rest day between sessions. Information about therapy content and patient compliance was determined using custom-made therapy journals, which were completed by therapists after each session. Sessions were held at children’s schools and/or in private practices. The main therapy components were progressive resistance exercises (PRE) based on current guidelines for typically developing children (17) and children with CP (i.e. intensity of 8–15 repetion maximum) (18) to improve strength and endurance, and functional goal-directed exercises with goals at the ICF activity level set by therapist and parents in dialogue. Due to large clinical heterogeneity, therapy content was individually tailored within the framework of the guideline, relying strongly on physiotherapists’ clinical reasoning abilities. All paediatric physiotherapists involved were experienced in treating children with CP. After the primary end-point measurements, PT reverted to individuals’ pre-study intensity.
In both intervention groups, 2–4 weeks of serial casting (i.e. below-knee walking casts changed weekly) could be prescribed in case of passive ankle dorsiflexion with extended knee less than 0°, starting approximately 1 week after iPT commenced (i.e. 2 weeks after BoNT-A), and ending when 0° dorsiflexion was possible. Therapy continued when children wore casts. If prescribed, (re)alignment of current or new AFOs was arranged as soon as possible.
Primary-end-point measurements were performed when individual 12-week iPT periods ended. Long-term follow-up measurements were completed 12 weeks thereafter (24 weeks). Independent assessors scored the clinical outcome measures and participants completed web-based questionnaires. Regarding assessment of safety and reporting of adverse events, all persons involved adhered to Good Clinical Practice (GCP) procedures.
Three outcome measures assessing gross motor function, physical activity levels and generic health-related quality of life (HRQoL) were used as primary effectiveness outcomes. Children with CP can experience a good quality of life despite having significant functional limitations (19).
Gross motor function was measured with the item set version of the Gross Motor Function Measure (GMFM-66), a widely used observational instrument that scores the capacity of children with CP to perform gross motor skills (16). The item set version (GMFM-66-IS) is reliable, valid and responsive for determining changes in gross motor function in CP (20).
Actual everyday physical activity levels were measured objectively using an ambulatory monitoring device (AM, Actigraph-GT3X+ 3D-accelerometer, 4.6 × 3.3 × 1.5 cm; 19 g, ActiGraph, Pensacola, FL, USA), validated for use in children with CP (21). Children wore the devices on an elastic belt positioned on the waist (on the less-affected side), and parents were instructed about donning and doffing the device. Devices were worn during the daytime for 7 days, except while showering/bathing or swimming. Accelerometer signals (sample frequency 30 Hz) were analysed using Actilife software (version 6.6.2, ActiGraph). For all 3 axes, activity counts were calculated using a 5-s epoch length, and from this, a vector magnitude was calculated. Periods of continuous zero counts lasting 15 min or longer were defined as non-wear periods (and were excluded from further analyses). Days with at least 480 min wear time were considered valid. The following outcome measures were calculated: total amount of activity counts per day (Total-counts), mean intensity of physical activity counts per min (CpM) and mean percentage of the day spent sedentary (%Sedentary, using Evenson cut-off points) (22).
HRQoL was measured using child self- and proxy-reported questionnaires. Functional health status was measured using the Child Health Questionnaire – proxy version (CHQ-PF28). The CHQ is a generic, norm-referenced HRQoL instrument that measures physical and psychosocial well-being of children approximately ≥ 5 years of age (23). The DISABKIDS questionnaire condition-specific CP module was used to measure the impact of this condition (24). The DISABKIDS-smiley self- and proxy-reported paediatric scales, in the form of ”emoticon faces”, were used for scoring HRQoL (24).
The commonly used preference-based Health Utilities Index (HUI), which assesses a number of different quality of life domains, was the main instrument for economic evaluation (25). The HUI-15Q 15-item proxy questionnaire was used to classify children to 2 complementary HUI health state classification systems by applying HUI2 and HUI3 multi-attribute utility formulas (25).
Economic evaluation was performed from a societal perspective (26) and included healthcare and patient costs. Data on healthcare use and patient time were obtained from standardized parent/caregiver diaries (for iPT compliance, data were double checked with therapists’ administrations), hospital- and pharmacotherapeutic-registration and information systems. To calculate the total intramural medical costs per BoNT-A treatment, we distinguished referral, consultations of multidisciplinary spasticity-teams, standardized gait analysis before and after treatment, pre-anaesthetic assessment, BoNT itself, injections under full anaesthesia, a 1-day hospital stay and post-treatment medical monitoring. For the most important cost items, unit prices were determined via micro-costing methods (27). This was based on a detailed inventory and measurement of all resources used (manpower, equipment, materials, housing and overhead). If no differences in effect between the 2 interventions were found, the economic evaluation converted to a cost minimization analysis (CMA).
First, the characteristics of participants and the different treatment components in the 2 intervention groups were compared using conservative non-parametric tests. Subsequently, comparative analysis of effectiveness of BoNT-A+iPT vs effectiveness of only-iPT at primary-end-point and follow-up were performed using linear mixed model analyses. In these intention-to-treat (ITT) analyses to estimate differences in treatment effectiveness we adjusted for the dependency of repeated observations in each subject (random intercept). We also adjusted for randomized/preferred treatment participation, number of previous BoNT-A treatments, age and GMFCS level. The latter is the most relevant in all discussions related to management of spastic CP (5). All statistical analyses were carried out using IBM-SPSS statistics 21; the level of statistical significance was set at p < 0.05.
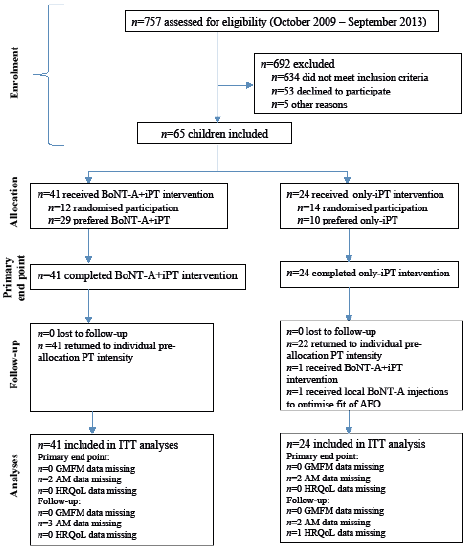
Between October 2009 and September 2013, 757 children were assessed for eligibility, of whom 84% did not meet the inclusion criteria, mainly because they were classified as GMFCS levels IV–V or they did not fit the age range (Fig. 1). Of 123 families who were invited to participate, 43% declined, primarily due to perceived additional burden. Finally, 65 children with spastic CP were enrolled, including 40% randomized participants. Within this latter group, 62% of families preferred 1 of the interventions (27% BoNT-A+iPT and 35% only-iPT). Overall, only 10 families (15%) were neutral regarding which intervention they received.
Fig. 1. Flow diagram of the SPACE BOP (SPAstic cerebral palsy; Cost-Effectiveness of BOtulinum toxin and Physiotherapy) study. BoNT-A: botulinum toxin type A; iPT: intensive physiotherapy PT: physiotherapy; ITT: intention-to-treat; AFO: ankle-foot orthoses; HRQoL: health-related quality of life; AM: Ambulatory Monitoring device; GMFM: Gross Motor Function Measure.
In total, there were 37 boys and 28 girls, mean age 7 years 4 months (standard deviation (SD) 2 years, 4 months). Fourteen participants had unilateral spastic CP subtype; 51 had bilateral spastic CP subtype; and 19, 23 and 23 children were classified as GMFCS levels I, II and III, respectively. There were no drop-outs and few missing data (Fig. 1).
Shortly after their baseline measurements, 41 children received BoNT-A+iPT and 24 children started only-iPT. In the 2 intervention groups, participants were evenly distributed over GMFCS levels, but in the only-iPT group there were more children with unilateral CP (explaining a smaller number of casting periods) and they were also younger (Table I).
Table I. Characteristics of participants and treatment components for the 2 intervention groups
The 2 intervention groups differed significantly regarding BoNT-A history (p = 0.002) and random participation (p = 0.021), both factors for which we planned to adjust in the comparative effectiveness analyses. Mean and SD number of injected BoNT-A units per kg bodyweight for children receiving BoNT-A+iPT were 9 (SD 5), 17 (SD 5) and 17 (SD 4), for GMFCS levels I, II and III, respectively. Comparison of baseline scores of the 2 intervention groups with conservative non-parametric tests showed that none of the outcome measures differed significantly. For various reasons, masking of their outcome assessor or physiotherapist accidentally failed before primary end-point was reached for 37% and 69% of the participants, respectively.
While adjusting for GMFCS level, BoNT-A history, age and randomized/preferred treatment allocation in the mixed models ITT analyses, at primary end-point (baseline to 12 weeks), we found only one statistically significant difference in treatment effect between intervention groups: AM-measured % of sedentary physical activity behaviour was in favour of only-iPT (Table II). At follow-up (baseline to 24 weeks), we did not find any statistically significant differences in treatment effects between the 2 interventions (Table II).
Table II. Linear mixed models analyses at the primary end-point (12 weeks) and follow-up (24 weeks)
The presence of only 1 statistically significant difference in effect between the 2 interventions (in favour of only-iPT), plus the absence of statistically significant differences for the Health Utility Index (HUI)-uti-mark3 and HUI-uti-mark2 utility scores, prompted us to change our economic evaluation into a cost-minimization analysis. Notably, however, the HUI-uti-mark3 and HUI-uti-mark2 utility scores all showed clinically meaningful improvements of ≥ 0.03 points (25) at the group level (n = 65) at both 12 and 24 weeks. The total cost per child for treatment up to primary end-point was significantly higher for BoNT-A+iPT than for only-iPT (8,963 vs 6,182 euro, p = 0.001, Table III). The mean difference in cost between the 2 interventions was 2,781 euro, of which 78% was related to BoNT-A procedures, 13% to iPT periods and 9% to casting and/or AFOs.
Table III. Cost comparison
There were no serious side-effects and/or adverse events related to BoNT-A and/or iPT, but casting periods and/or (re)alignment of AFOs were complicated in a number of cases (Table I). Because the proportion of children with casting periods nearly differed significantly between groups, we performed a post-hoc analysis adjusting for the presence/absence of casting periods in the mixed models; however, this did not change the present findings.
There is an international consensus that BoNT-A should not be used as stand-alone treatment; adjunctive interventions to lower extremity BoNT-A injections, such as casting, orthotic management and especially a period of (intensive) PT, are essential components of post-BoNT-A care (4). However, historically, BoNT-A is the actual adjunctive intervention (5). Therefore, we explicitly studied the added value of multi-level BoNT-A injections preceding a period of individually tailored iPT (which was equally intensive in both intervention groups) and the co-interventions casting and/or AFO (which were prescribed employing the same policy in both intervention groups) on clinical outcome at the higher ICF levels. With one exception in favour of only-iPT (AM-measured percentage of sedentary physical activity behaviour), we did not find statistically significant differences between the BoNT-A+iPT and only-iPT interventions for primary effect outcomes, whereas the mean treatment costs per child were significantly higher for BoNT-A+iPT.
Previous studies have discussed the uncertainty regarding the degree to which positive effects of combined BoNT-A and iPT could be attributed to BoNT-A or to higher intensity of PT (7–9). Debate regarding the optimal BoNT-A dose is ongoing (4, 5, 28), and recommendations regarding the ideal dose remain expert-based. In our study, the medical specialists had ample experience with BoNT-A, and they applied the maximum recommended BoNT-A doses per large muscle group. Adjunctive casting and/or (re)alignment of AFOs are part of usual care, but are not necessary for every child with spastic CP. The proportion of children who had problems with their cast(s) during the iPT period was somewhat higher in the only-iPT treatment group; however, casting in the BoNT-A+iPT group did not add to improved effectiveness of combined treatment at the group level.
Critical appraisal of the literature regarding the effectiveness of BoNT-A shows that research questions have mainly been based on an implicit assumption that BoNT-A is the most active component in combined treatment periods. Positive clinical experiences with combined BoNT-A and other therapies may have been unjustly attributed to BoNT-A injections. This may also explain the difficulties in randomization that we and others (29) experienced, exacerbated by BoNT-A safety discussions preceding our study (6).
As iPT appears to be the dominant component for effectiveness in our study, future research should also focus on how to optimize PT content and planning. Currently there is little evidence regarding how to organize PT to be optimally cost-effective (4, 5, 10). The large heterogeneity in spastic CP emphasizes that individualized assessment and treatment are indeed essential (28). However, lack of added value of BoNT-A at the group level does not necessarily imply that children with CP cannot benefit from the injections. There may be a subgroup within the CP population and/or particular treatment outcomes for which BoNT-A is of added value. This would probably be more easily identified by setting up CP patient registries. As stated by Damiano, it is important not only to focus on mean group results, but to design studies that provide insight into what works for which groups of patients (30).
The main limitations of the current study were its pragmatic design, with 40% randomized participants, and the relatively small sample size of 65 children. A fully randomized controlled trial with a larger number of participants would have been more optimal, including for the economic evaluation. However, there are practical limitations to randomized controlled trials in rehabilitation research (12, 13, 31). It was difficult to convince parents to permit their children to participate randomly because of the strong preferences for one of the interventions (which we found surprising since we compared 2 ”fully fledged” interventions). Once in the study, however, families were highly motivated, which resulted in zero drop-outs and very few missing data, both adding to statistical power. It has to be noted, however, that our original power calculations may not have been completely valid for the present number of participants and the distribution across intervention groups. In addition, blinding of outcome assessors and physical therapists accidentally failed for a number of participants, which is a typical difficulty inherent to this type of research (4). Large heterogeneity (even within this subgroup) of the CP population also limits the feasibility of tightly controlling an intervention.
As shown in Table I, there were some imbalances between the larger group that received BoNT-A+iPT and the smaller group that received only-iPT, which may have introduced some bias. Having more severe spastic CP and being older increased the chances of a more extensive BoNT-A history, which may have been perceived as (un)pleasant, thereby explaining preferences, and objections to randomization. It appeared more difficult to identify and enrol participants who preferred only-iPT because BoNT-A+iPT is a generally accepted and most commonly prescribed treatment combination for ambulatory children with spastic CP. We note that it has been reported that receiving preferred treatment does not affect outcomes (32).
For multicollinearity and to maximize statistical power, we only adjusted for BoNT-A history, GMFCS level, age and (non-)randomized participation in the comparative analyses. Of course, we realize that the latter adjustment is debatable from a statistical point of view. Unfortunately there were no children with GMFCS
level III in the randomized BoNT-A+iPT subgroup. This was due to a blockwise randomization scheme stratified by GMFCS level per measuring location, with a block length of 4 in the first block and a length of 2 in subsequent blocks. Consequently, baseline differences between the 2 intervention groups were larger for randomized participants than for non-randomized participants. For this reason, and because there were no differences between the 2 intervention groups regarding their baseline scores and the most important patient and treatment characteristics, it was considered justified to perform analyses of BoNT-A+iPT vs only-iPT with all participants in one comparison. However, because these issues may limit interpretability of our findings, we strongly advocate additional research into the added value of BoNT-A to confirm our findings. The fact that all intervention-related procedures largely resembled routine practice in the Netherlands and that a subgroup was given their preferred treatment adds to the generalizability of results. However, it remains unclear to what degree improvements in our study over time were related to natural development, as we did not have a control group without intervention.
To our knowledge, this industry-independent study is the first to specifically study the added value of BoNT-A injections in a widely used treatment combination, with equally highly intensive periods of physiotherapy, and, if necessary, adjunctive casting and/or AFOs in both intervention groups. In conclusion, at the group level, BoNT-A injections do not improve clinical effect outcomes compared with iPT alone and are not cost-effective. Thus, both from a clinical and an economic viewpoint, it is time to critically reconsider the use of BoNT-A injections in treatment aiming at improving gross motor function, physical activity levels and/or HRQoL of 4–12 year-old children with spastic CP.
The authors greatly appreciate the Netherlands Organisation for Health Research and Development (ZonMW grant number: 170995003) and Rijndam Rehabilitation Centre for their financial support. The authors thank the SPACE BOP study group members, Dr Herwin Horemans, Emiel Sneekes, Eline Bolster, Irma Viola, Karlijn van Beek and Johannes Verheijden, for their substantial contributions to the study. The authors also thank Gerard Borsboom (statistical advice); Dr Wim Hop (randomization scheme); Everett Claridge (English language editing); Kim van Hutten (measurements); Dr Eugene Rameckers (iPT guideline); rehabilitation physicians of VU Amsterdam, Erasmus MC Rotterdam, Rijndam Rehabilitation Rotterdam; and the secondary centres in the Amsterdam region, Revant Breda, Libra Rehabilitation & Audiology Eindhoven, De Hoogstraat Utrecht and De Trappenberg Huizen (patient enrolment), all physical therapists, casting room workers, CPOs and, finally, the participating children and their families. This article has been handled by Editor-in-Chief Kristian Borg.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize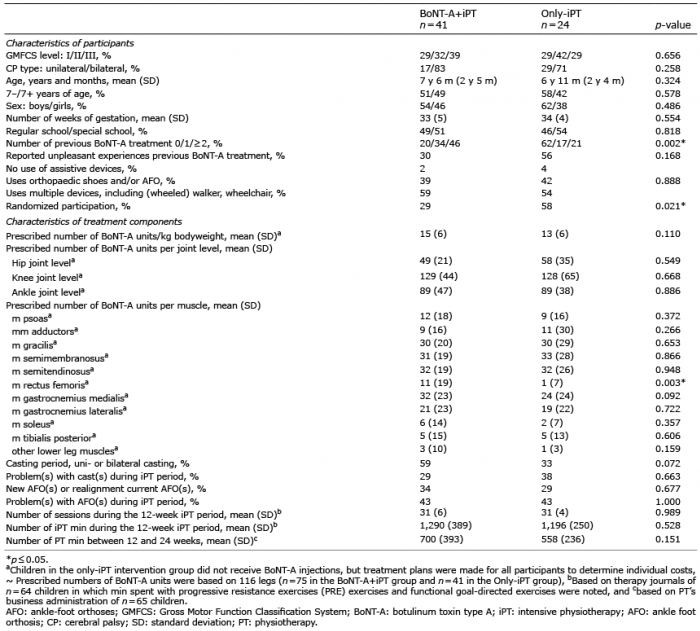 Click to show fullsize
Click to show fullsize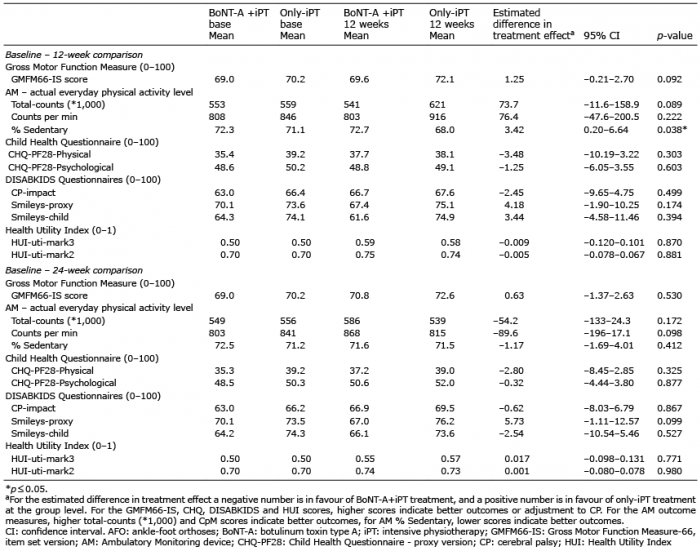 Click to show fullsize
Click to show fullsize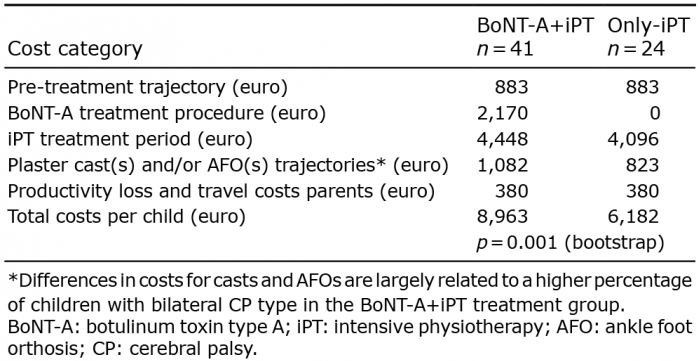 Click to show fullsize
Click to show fullsize